Female health
8 mins read
Written by Forth
December 22, 2021
The occurrence of endometriosis in postmenopausal women has been cited in medical literature as being between 2% and 5%. A retrospective study of over 42,000 women who underwent surgical treatment for endometriosis found that 17% were perimenopausal and 2.5% were postmenopausal.
Endometriosis is a medical condition that affects around 176 million women worldwide and 1 in 10 women in the UK . It occurs when the tissue (endometrial cells) that lines the uterus grows elsewhere in the body such as the ovaries, bowel, fallopian tubes, and bladder. This can cause a wide range of symptoms including severe and chronic pain that can be disruptive to everyday life. While the exact cause of endometriosis is not yet fully understood, scientists and medical professionals have been working tirelessly to uncover the factors that contribute to its development.
The exact cause of endometriosis is not fully understood, although there have been recent breakthroughs in diagnosis and better treatment.
For example, there is now an endometriosis saliva test that measures 109 different microRNAs to provide a positive or negative result for the condition. Studies have shown a link between dysregulation of certain microRNAs and endometrial lesions.
There has also been a potential breakthrough that could lead to improved treatment of endometriosis.
However, the factors listed below are thought to play a role in the development of endometriosis.
Genetics: Studies have shown that women with endometriosis are more likely to have a family history of the condition[1]. This suggests that there may be a genetic component to endometriosis. However, the exact genes involved are not yet known.
Immune system: Some experts believe that endometriosis may be caused by an abnormal immune response to tissue that has travelled outside the uterus. This tissue is thought to be seen as foreign by the immune system, which then attacks it.
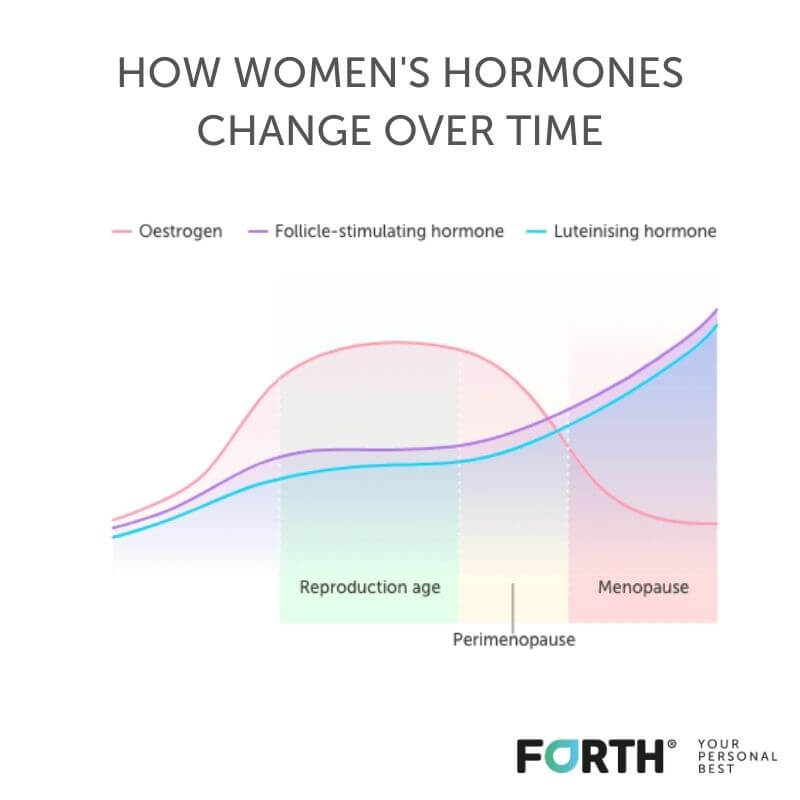
Hormones: The hormones oestrogen and progesterone are thought to play a role in the development of endometriosis. Oestrogen is thought to promote the growth of endometrial tissue, while progesterone may help to suppress it.
It is thought that unvarying levels of oestrogen from HRT may support the growth of endometriotic lesions, but the data surrounding HRT and endometriosis is limited, with little evidence to say endometriosis returns when women begin taking HRT.
HRT has many benefits to longer term health, such as reducing the risk of heart disease and osteoporosis, so should be consider within the context of other conditions.
Environmental factors: Some studies have suggested that exposure to certain chemicals or pollutants may increase the risk of endometriosis[2]. However, more research is needed to confirm this link.
Retrograde menstruation: This is where menstrual blood flows back through the fallopian tubes and into the pelvic cavity, rather than leaving the body. The menstrual blood contains endometrial cells which can stick to the pelvic walls.
Metaplasia: Metaplasia is where one cell type can turn into a different type of cell. It usually happens in response to inflammation and allows cells to better adapt to their surrounding environment. It may help to explain why endometriosis cells appear in other parts of the body or why some men develop them when they take certain hormonal treatments [3].
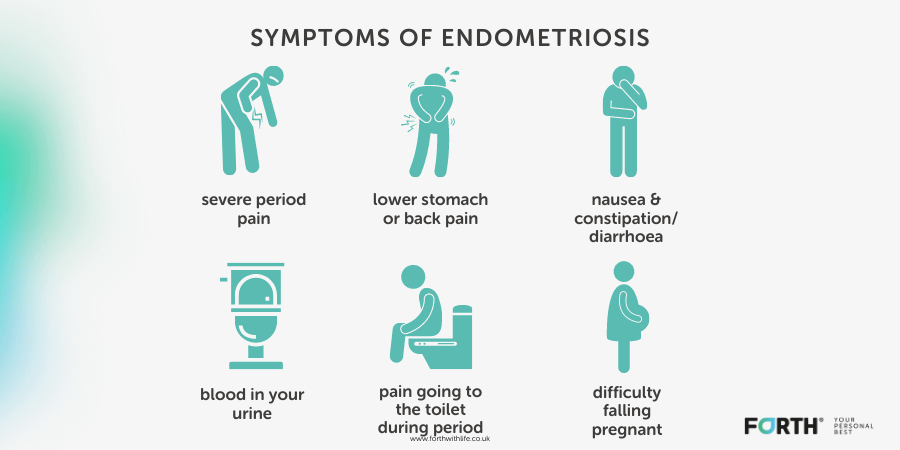
The symptoms of endometriosis can vary from woman to woman. Some women may experience mild symptoms, while others may experience severe symptoms. The most common symptoms of endometriosis include:
Some of the most common risk factors for endometriosis include:
The diagnosis of postmenopausal endometriosis is challenging, not least because it is rare. The gold standard for diagnosing endometriosis, regardless of age, is a laparoscopy. This is where a small camera is inserted into the stomach to inspect the pelvis for evidence of endometriosis lesions.
There are three options for treating endometriosis at any age, these are:
Surgery to remove endometriosis and cysts via keyhole surgery. In some cases, more complex surgery is required if the bowel or bladder are affected, as well as a hysterectomy to remove the womb or a oophorectomy to remove the ovaries.
There is more information on surgical treatments at Endometriosis UK.
There are various hormone treatments for endometriosis to suppress the production of oestrogen. However, this isn’t generally needed in postmenopausal women as oestrogen levels have declined.
Learn more about hormone treatment.
There are pain relief and management options for endometriosis in the form of pain killers, heat applications, physiotherapy and pain clinics.
Learn more about pain relief.
Living with endometriosis can be challenging, but there are things you can do to manage the symptoms and improve your quality of life.
Diet
One of the most effective ways to manage endometriosis is by eating a healthy, balanced diet. This means consuming plenty of fruits, vegetables, whole grains, and lean protein sources while limiting processed foods, sugar, and saturated fats. A healthy diet can help reduce inflammation in the body, which can in turn reduce the severity of endometriosis symptoms.
Exercise
Regular exercise is also important for managing endometriosis symptoms. Exercise can help reduce stress, improve mood, and boost overall health and wellbeing. Low-impact exercises like yoga, swimming, and walking are great options for women with endometriosis, as they are less likely to cause pain or discomfort.
Stress Reduction
Reducing stress is another key component of managing endometriosis. Stress can exacerbate symptoms and make them more difficult to manage. Finding ways to relax and unwind, such as through meditation, deep breathing exercises, or spending time in nature, can help reduce stress levels and improve overall well being.
Get Support
It is also important to seek support from friends, family, and healthcare professionals. Endometriosis can be a difficult condition to live with, and having a strong support system can make all the difference. Joining a support group, talking to a therapist, or seeking advice from a healthcare professional can all be helpful for managing endometriosis symptoms.
Endometriosis after the menopause is thankfully rare, but more needs to be done to not only diagnose the condition sooner in women of reproductive age, but to also carry out more research into endometriosis postmenopause.
This will enable women to get the right treatment and support and would allow women to have more informed discussions around the treatment of their postmenopause symptoms in light of previous endometriosis.
Gemmell, L, C et al. (2017). The Management of Menopause in Women with A History of Endometriosis: A Systematic Review. Human Reproduction Update: 23(4), pp 481-500.
Garcίa Manero, M et al. (2009). Endometriosis in a Postmenopausal Woman Without Previous Hormonal Therapy: A Case Report. Journal of Medical Case Reports: 3(135).
Chantalat, E et al. (2020). Estrogen Receptors and Endometriosis. International Journal of Molecular Sciences: 21(8).
Shah, D. (2014). Postmenopausal Endometriosis: An Enigma Revisited. J Midlife Health: 5(4), pp 163-164.
Like this article? Here are some more based on similar topics.