AutoDraw

Menopause Test
For women who have reached menopause. Checks key hormones alongside bone health and heart health.
20 Biomarkers
£129
8 mins read
Osteoporosis, often called "brittle bone disease," weakens bones and increases fracture risk, affecting millions, especially postmenopausal women. This blog covers its causes, symptoms, prevention, and treatment, offering key insights for maintaining strong bones and supporting bone health at any age—helping you stay active and resilient longer.
Written by Dr Thom Phillips
October 1, 2025

Osteoporosis is a systemic skeletal disorder that affects millions of people across the UK.
The condition is characterised by low bone mass and the micro-architectural deterioration of bone tissue, which leads to increased bone fragility and a consequent increase in fracture risk.
While some loss of bone density is a normal part of the ageing process, osteoporosis is a disease state where this loss is significant enough to cause bones to become weak and brittle. It is frequently referred to as a “silent disease” because it typically presents no obvious symptoms until a bone breaks, often following a minor fall or impact.[3] These fractures most commonly occur in the hip, spine, or wrist, and can lead to chronic pain and long-term disability.[5]
The condition often begins with a milder form of bone density loss known as osteopenia. This is not yet osteoporosis, but it is considered a precursor to the disease, as a person’s bone density is lower than normal. Not everyone with osteopenia will develop osteoporosis, and lifestyle changes can help to prevent its progression.
A common point of confusion for many people is the difference between osteoporosis and osteoarthritis. While both conditions affect the musculoskeletal system, they are fundamentally distinct in their underlying cause and effects.[5]
Osteoporosis primarily affects the density and strength of the entire skeleton, making bones porous and prone to fractures.
In contrast, osteoarthritis is a joint disease caused by the gradual breakdown of cartilage over time, leading to pain, stiffness, and reduced mobility in specific joints, such as the knees, hips, and hands. Osteoporosis itself does not cause pain unless a fracture has occurred. The table below provides a concise overview of these differences to help clarify this common misconception.
| Feature | Osteoporosis | Osteoarthritis |
| Primary Issue | Loss of bone mass and density | Breakdown of joint cartilage |
| Affected Area | The entire skeleton, particularly the spine, hips, and wrists | Specific joints, most commonly the knees, hips, and hands |
| Pain | Not painful until a fracture occurs | A primary symptom, causing chronic joint pain and stiffness |
| Cause | Disruption of bone remodelling; failure to produce new bone | Gradual “wear and tear” from ageing, overuse, or injury |
| Effect on Bones | Bones become porous, weak, and brittle | Bone spurs may develop at joint edges, but bone itself is not porous |
To understand osteoporosis, it is helpful to first understand the natural process of bone remodelling.
Throughout life, bone is a living tissue that is constantly being broken down by cells called osteoclasts and rebuilt by cells called osteoblasts. This process ensures the skeleton remains strong and healthy.
From a person’s late twenties to early thirties, bone mass typically peaks, and the rate of bone formation and breakdown reaches a state of near equilibrium.8 However, as people age, the rate of breakdown begins to outpace the rate of formation, leading to a natural decline in bone density.
Osteoporosis occurs when this decline is accelerated or becomes significantly pronounced, resulting in weakened, fragile bones.
Several factors contribute to a person’s risk of developing osteoporosis. These can be broadly divided into those that cannot be changed and those that can.
Age and Gender
Ageing is the primary cause of osteoporosis, as bone density naturally decreases from the fourth decade of life onwards.[4] Women are at a significantly higher risk than men, accounting for approximately four out of every five cases.[3] This is largely due to the rapid decrease in oestrogen levels through perimenopause and into menopause, as this female hormone plays a crucial role in maintaining bone strength.[3] Men also experience a gradual decline in bone strength as they age, typically from the age of 60 to 65, when testosterone levels decrease.
Genetics and Body Frame
A person's genetic makeup determines the potential size and strength of their skeleton. An individual is at a greater risk of developing osteoporosis if they have a family history of the condition or if a parent has fractured a hip.[6] Men and women who have small body frames tend to have less bone mass to draw from as they age, which increases their risk.[6]
Lifestyle
A sedentary lifestyle, smoking, and excessive alcohol consumption all contribute to bone loss.3 Smoking can slow down the activity of bone-building cells and may also lead to earlier menopause in women, further accelerating bone loss. Excessive alcohol intake can interfere with the absorption of essential nutrients for bone health and also increases the risk of falls and subsequent fractures.[4] Low body weight is also a risk factor, as it is associated with smaller, more fragile bones and less fat padding to protect against falls.[10]
Medical Conditions and Medications
Several chronic medical conditions are known to affect bone strength. These include rheumatoid arthritis, hyperthyroidism, Crohn's disease, and coeliac disease.[10] Additionally, the long-term use of certain medications, such as oral corticosteroid tablets (steroids) and some anti-epileptic or cancer treatments, can negatively impact bone density.[10]
We looked at thousands of blood test results in September 2025 and uncovered how perimenopause & menopause impact bone health.
Using our HealthCoachTM scores, we found that the median Bone & Muscle Health scores are:
Men: 75/100
Women: 68/100
Our Bone & Muscle Health score is generated from blood test results for the following components:
ALP - a measure of whether bone turnover is accelerated
Calcium - Crucial component of bone
Magnesium - About 60% of the body's total magnesium is stored in the skeleton, making it a vital component for bone strength.
Sex Steroid Hormones - testosterone for men, oestradiol (oestrogen) for women
Vitamin D - Vitamin D helps regulate bone turnover by stimulating calcium absorption from the gut and working with parathyroid hormone (PTH) to maintain proper calcium levels
Each component is scored between 1 and 100, with 100 being the best achievable score. The results show that hormones play a much larger role in muscle & bone health than markers like calcium, magnesium and vitamin D.
Both men and women had scores in the healthy range (75 or higher) for ALP, calcium and CK, with women scoring over 75 for magnesium. However, the median Sex Steroid Hormone score for women (62) is 31 points lower than the men’s score (93).
| Table 1: Median Component Scores by Sex | ||
| Component | Women | Men |
| ALP | 92 | 95 |
| Calcium | 94 | 95 |
| CK | 93 | 89 |
| Magnesium | 77 | 67 |
| Sex Steroid Hormones | 62 | 93 |
| Vitamin D | 63 | 61 |
Digging into this score in more depth, we can see a sharp drop off in scores in women over 40 – around the time many women enter perimenopause and experience symptoms related to shifting hormone levels.
The median Sex Steroid Hormone score for women peaks at 80 in their early 30s, but drops to just 9 by their 60s – an 89% decline. Meanwhile, men’s scores remain stable.

So what causes this drop in women?
We looked at over 27,000 blood test results and discovered that declines in oestrogen (oestradiol) levels, related to perimenopause and menopause, cause the steep drop in Sex Steroid Hormone scores.
| Table 2: Median Sex Steroid Hormone Scores & Oestrogen Levels in Women | ||
| Age | Median Sex Steroid Hormone Score | Median Oestrogen Level |
| 18-20 | 66 | 113 |
| 21-25 | 68 | 131 |
| 26-30 | 75 | 145 |
| 31-35 | 77 | 149 |
| 36-40 | 80 | 170 |
| 41-45 | 79 | 201 |
| 46-50 | 69 | 234 |
| 51-55 | 46 | 191 |
| 56-60 | 15 | 63 |
| 61+ | 9 | 32 |

We looked into whether HRT has an impact, and found that, despite higher oestrogen levels in women using HRT, a similar trend persists in declining levels as women age.
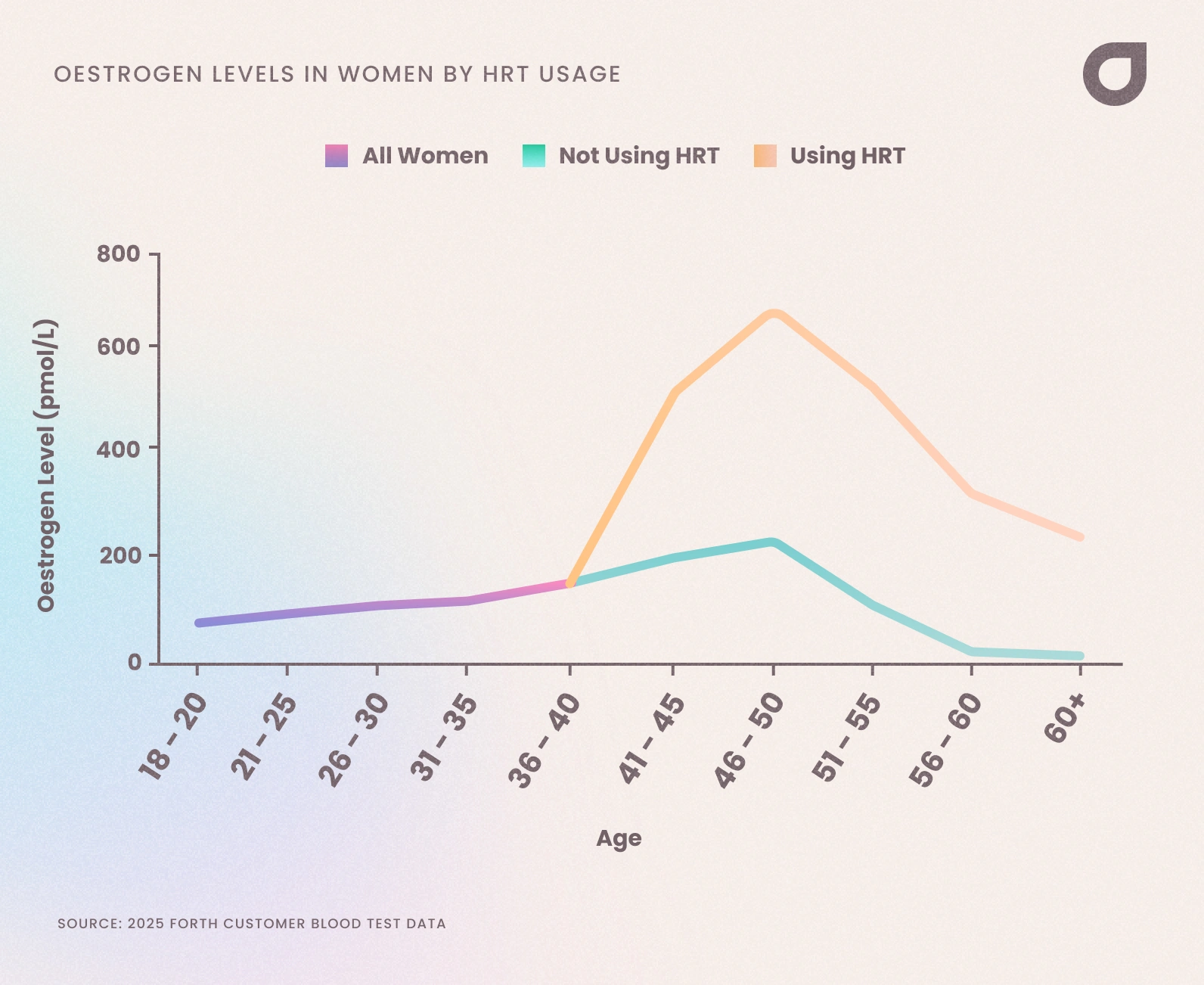
This highlights the benefits to women of using HRT to boost hormone levels and prevent conditions like osteoporosis, along with other benefits, such as lessening symptoms like hot flushes, night sweats and anxiety.
"Oestradiol plays a crucial role in maintaining bone density throughout a woman's life. During perimenopause and postmenopause, declining oestradiol levels significantly accelerate bone loss, increasing osteoporosis and fracture risk. It’s estimated that half of women over 50 years will have a low trauma fracture due to osteoporosis. Over half a million people need hospital treatment every year for fragility fractures - which means they broke a bone by just falling over from standing!
Oestradiol protects bone health by inhibiting osteoclasts (cells that break down bone) while supporting osteoblasts (cells that build bone). This maintains the delicate balance of bone remodelling. When oestradiol levels drop during menopause, bone resorption outpaces formation, leading to decreased bone mineral density—women can lose up to 20% of their bone density in the five to seven years following menopause.
The most vulnerable sites include the spine, hips, and wrists, where fractures can cause substantial morbidity and mortality. Hormone replacement therapy containing oestradiol effectively prevents this accelerated bone loss and reduces fracture risk. For women at high osteoporosis risk, maintaining adequate oestradiol levels through HRT, alongside calcium, vitamin D, and weight-bearing exercise, represents a key preventive strategy for preserving skeletal health and independence in later life.
"
Because osteoporosis is a “silent disease,” the early stages are typically asymptomatic.[3] The first indication that a person has the condition is often a fragility fracture, a broken bone resulting from a minor fall or impact that would not normally cause a fracture in a healthy person.
As the condition progresses, or after multiple fractures have occurred, certain symptoms may become noticeable. These can include persistent or severe back pain from fractured or collapsed vertebrae in the spine, a gradual loss of height, and the development of a stooped posture, sometimes referred to as a “dowager’s hump”.[3] These changes are a direct result of the bones becoming so weak that they can no longer support the body’s structure.[6]
The gold-standard diagnostic tool for osteoporosis is a DEXA (dual energy X-ray absorptiometry) scan.[3] This simple, non-invasive scan measures a person’s bone mineral density (BMD), which is then compared to the average BMD of a healthy young adult to produce a T-score.
There is a common misconception that osteoporosis has distinct numbered stages, such as “5 stages”.[8] However, this is not a medically recognised staging system. Instead, doctors use the T-score from a DEXA scan to classify bone health into one of three categories, which reflect the differing levels of severity:
Normal Bone Density: A T-score of -1.0 or above
Osteopenia: A T-score between -1.0 and -2.5. This indicates bone density that is lower than normal and is considered a precursor to osteoporosis.[3]
Osteoporosis: A T-score of -2.5 or below. At this stage, bone density is significantly reduced, and the risk of fracture is high.[3]
"Fragility fractures (broken bones with underlying bone thinning) are a massive health issue/ As well as being hugely inconvenient, often we can use a fragility fracture as a marker of overall health and, perhaps surprisingly, having a fragility fracture doubles the risk of death in the following year for older women and triples the risk in older men."
Blood tests can provide a different and complementary picture of bone health. They are used to check for underlying mineral and vitamin deficiencies that may be contributing to bone loss, to rule out other conditions that can affect the skeleton, and to monitor the effectiveness of treatment over time.[16]
A standard “bone screen” blood test typically measures several key biomarkers, each providing valuable information about the complex processes involved in bone health and metabolism.
Calcium and Corrected Calcium
Calcium is the primary mineral that gives bones their strength and structure.[20] A blood test measures the total amount of calcium in the blood. However, since much of this calcium is bound to a protein called albumin, you should also check your corrected calcium, which accounts for the albumin level to provide a more accurate reflection of the "active" calcium available for biological processes.[21] Abnormal levels may signal issues with the parathyroid glands or kidney function.[18]
Vitamin D (25-Hydroxy Vitamin D)
This is perhaps one of the most important biomarkers for bone health, as vitamin D is essential for the body's absorption of calcium.20 Low levels of vitamin D can lead to bone softening, a condition known as osteomalacia, and contribute to osteoporosis.[16]
Alkaline Phosphatase (ALP)
ALP is an enzyme found in high concentrations in the liver and bones. In the context of bone health, it plays a key role in the mineralisation process. Elevated levels can indicate increased bone turnover, which may be a sign of a healing fracture, Paget's disease, or other metabolic bone disorders.[16]
| Biomarker | Function in Bone Health | What Abnormal Levels May Indicate |
| Calcium | Essential for bone strength and density | Kidney disease, parathyroid disorders, or other bone disorders 18 |
| Phosphate | Works with calcium to build bone structure | Kidney disease or nutritional imbalances [18] |
| Vitamin D | Crucial for calcium absorption and bone formation | Deficiency, which can lead to bone softening (osteomalacia) or contribute to osteoporosis [16] |
| Alkaline Phosphatase (ALP) | An enzyme involved in bone mineralisation | Increased bone turnover due to Paget’s disease, healing fractures, or other bone disorders [16] |
A diagnosis of osteoporosis is a life-changing event, but it is important to understand that the condition can be effectively managed. A common question is whether osteoporosis can be reversed or cured. The short answer is that it cannot be completely reversed or cured, but with a combination of health and lifestyle adjustments and appropriate medical treatments, it is possible to slow or stop bone loss and, in some cases, even rebuild bone density.[8]
The management of osteoporosis involves a multi-pronged approach tailored to your individual needs.
Medical treatment primarily aims to keep bones as strong as possible and to reduce the risk of fractures. There are two main categories of medication:
Anti-resorptive drugs
These medications work by slowing down the rate at which bone is broken down. The most common type is bisphosphonates (e.g., alendronic acid, risedronate), which are typically taken as tablets or injections.[4] Other options include selective oestrogen receptor modulators (SERMs), such as raloxifene, which mimic the protective effects of oestrogen on bone.[4]
Bone-building drugs
In more severe cases of osteoporosis, especially when other treatments have not been effective, a doctor may prescribe treatments that actively stimulate cells to create new bone. Examples include teriparatide and romosozumab.[4]
For menopausal women, Hormone Replacement Therapy (HRT) may also be an option to help control symptoms and keep bones strong.[11]
Physiotherapy can also play a crucial role by providing targeted exercises and pain management strategies to improve mobility and reduce symptoms.
"Although many people will view a broken bone as a painful problem, many do not consider it to be a life threatening or life limiting condition. However, around 50% of people who break a hip are unable to live completely independently following the injury and perhaps more worryingly, around 10% of people die within a month of breaking a hip, with 30% dying within a year. This shows that bone health is also a sensitive barometer of overall health status."
A healthy diet is a cornerstone of bone health, both for prevention and management. Two key nutrients are particularly important: calcium and vitamin D.[20]
The Best Foods for Bones
The recommended daily intake for adults in the UK is 700 milligrams of calcium, which can often be achieved through a varied diet. Excellent sources include dairy products (milk, cheese, yoghurt), leafy green vegetables like broccoli and kale, dried fruit (figs, raisins, apricots), tofu, and fish with edible bones, such as sardines.11 Vitamin D is crucial for helping the body absorb calcium. While most vitamin D is produced by the skin's exposure to sunlight, dietary sources include oily fish (salmon, mackerel, sardines), egg yolks, and fortified foods like some cereals and plant-based milks.[20] The NHS recommends that everyone in the UK consider taking a daily vitamin D supplement during the autumn and winter months, as sunlight is not strong enough to produce adequate amounts.[20]
Foods and Drinks to Limit
Certain dietary choices can be detrimental to bone health. A high intake of sodium, often found in processed foods and ready meals, can lead to increased calcium excretion through the urine, which may weaken bones over time.[27] Similarly, excessive consumption of caffeinated beverages can interfere with calcium absorption.[28] Excessive alcohol consumption is also strongly linked to bone loss, as it can interfere with the body's ability to absorb calcium and may alter hormones that help keep bones strong.[10] While a balanced diet is important, extremely high-protein diets may lead to calcium loss through urine, and some soft drinks, particularly colas, contain phosphoric acid which has been linked to lower bone density.
| To Consume Regularly | Reason |
| Dairy, leafy green vegetables, dried fruit, fortified foods, canned fish with bones | Rich in calcium, the main building block of bones |
| Oily fish, egg yolks, fortified cereals | Good sources of vitamin D, which aids calcium absorption |
| To Limit or Avoid | Reason |
| High-sodium foods (processed meals, snacks, canned soups) | Can increase calcium excretion through urine, weakening bones |
| Excessive alcohol | Interferes with nutrient absorption and increases fall risk |
| Excessive caffeine | Can interfere with calcium absorption |
| Soft drinks | Phosphoric acid has been linked to lower bone density |
Regular physical activity is an essential component of both preventing and managing osteoporosis. It helps to build and maintain bone and muscle strength, improves balance, and can significantly reduce the risk of falls and subsequent fractures.[3]
The best types of exercise for people with osteoporosis are those that put some degree of stress on the bones to stimulate new bone formation, without placing them at risk of fracture.
Weight-bearing activities
These exercises work directly on the bones in the legs, hips, and lower spine to slow bone loss. Examples include brisk walking, dancing, stair climbing, and gardening.[30]
Muscle-strengthening exercises
Activities like weight lifting and yoga help build and maintain muscle mass, which provides better support for the skeleton.
Balance and flexibility exercises
Improving balance is crucial for reducing the risk of falls, a major concern for those with reduced bone density. Specific physiotherapy-led exercises can be highly beneficial.
"Regular, weight bearing exercise, as well as strength based exercise is probably the most important thing you can do to look after your bone health. Minimise the time you sit on a daily basis as even standing can be beneficial. The Royal Society of Osteoporosis ha ssome excellent resources regarding exercise if you've already been diagnosed with Osteoporosis. "
The Royal Society of Osteoporosis has some excellent resources for understanding how to build up your exercise if you’ve been diagnosed with Osteoporosis or Osteopenia.
Equally important for those with osteoporosis is knowing which exercises to avoid to prevent a fracture.
High-impact exercises
Activities such as running, jogging, and jumping put excessive force on weakened bones and can lead to fractures.[32]
Spinal flexion and twisting
Movements that involve forward bending or excessive twisting of the spine should be avoided. This includes exercises like crunches, sit-ups, and certain yoga or Pilates poses. These movements can cause compression fractures in the vertebrae, which are highly susceptible to fracture in people with low bone density.
Jerky, rapid movements
Sudden, unpredictable movements should be avoided in general to minimise the risk of falls and injuries.
| Osteoporosis-Friendly Exercise Guide | |
| Recommended Activities | Exercises to Avoid |
| Brisk walking, dancing, stair climbing, hiking | High-impact activities like jogging and jumping |
| Light weight lifting, resistance training | Exercises involving spinal flexion (crunches, sit-ups, forward bends) |
| Yoga, Pilates (with modifications), Tai Chi | Movements involving excessive twisting or jerky, rapid motions |
| Balance and flexibility exercises | Sports with high fall or impact risk (e.g., skiing, snowboarding) |
There are no official, medically recognised “stages” of osteoporosis.[8] Instead, doctors use a T-score from a bone density scan to classify a person’s bone health as normal, osteopenia (low bone density), or osteoporosis. This classification, along with other risk factors, guides treatment decisions. The misconception of “stages” may stem from the progressive nature of the disease, but it is not a clinical term used in diagnosis.
Osteoporosis itself is not a terminal illness and does not directly shorten a person’s lifespan.[15] The primary risk to life expectancy comes from the complications of the disease, specifically fractures. Hip fractures in older adults, in particular, can lead to a significant increase in mortality, often due to associated complications. Research has shown that with proper treatment, a person can live for many years following their diagnosis, and survival rates are good when the condition is managed effectively.
In the UK, osteoporosis is a recognised chronic illness, but it is not classified as a disability in itself. Eligibility for disability benefits, such as the Personal Independence Payment (PIP) or Employment and Support Allowance (ESA), is determined by the impact of the condition on a person’s daily life and ability to work, not by the diagnosis alone.[35] For example, if recurring fractures, chronic pain, or limited mobility from osteoporosis prevent a person from working or caring for themselves, they may qualify for support.[35]
The condition itself does not directly cause fatigue. However, a person with osteoporosis may experience tiredness due to related factors. This could include a vitamin D deficiency, which is known to cause fatigue, or persistent pain from fractures. The psychological and physical burden of managing a chronic condition can also contribute to feelings of tiredness.
Yes, osteoporosis can affect oral health.[39] A reduction in jawbone density, which is a common effect of osteoporosis, can lead to serious dental issues, including loose teeth and tooth loss.[39] It can also make a person more susceptible to periodontal (gum) disease, which further destroys the structures supporting the teeth. It is also worth noting that bisphosphonate medications, which are a common treatment for osteoporosis, have been linked to a rare but serious condition called osteonecrosis of the jaw (ONJ).
Our Menopause Health Blood Test is designed for women who have already reached menopause (12+ months without a period). Your sample is analysed by an accredited NHS laboratory in the UK, ensuring reliable and accurate results. This test helps you monitor key female hormone levels, including oestrogen and progesterone, as well as important biomarkers for bone strength and heart health – two areas of increased risk after menopause. It’s also an effective way to assess how well your HRT is working, helping you make informed decisions about your treatment and overall well-being.
AutoDraw
For women who have reached menopause. Checks key hormones alongside bone health and heart health.
£129
Thom works in NHS general practice and has a decade of experience working in both male and female elite sport. He has a background in exercise physiology and has published research into fatigue biomarkers.

Dr Thom Phillips
Chief Medical Officer
Like this article? Here are some more based on similar topics.