Hormonal Contraception: What are they and what are the side effects
Written by
Forth
December 2, 2024
In this article:
What is Hormonal Contraception?
Hormonal birth control are synthetic versions of the female hormones, progesterone and oestrogen, either in combination or progesterone-only.
There are a range of different hormonal contraceptives available and finding the best type for you will depend on your lifestyle and preferences. All types of hormonal birth control work to prevent pregnancy.
These are the different hormonal contraception types:
Oral contraceptives (‘the pill’ and the ‘mini-pill’) are the most common single type of contraception used in the UK with 42% of women using the pill[2].
How do they work?
Hormonal contraceptives prevent the natural menstrual cycle by maintaining consistent levels of oestrogen and/or progesterone to prevent ovulation, thickening the cervical mucus to stop sperm from entering the womb and fertilising an egg; as well as thinning the lining of the womb to lower the chances of a fertilised egg implanting and developing.
Which one is right for you?
The type of hormonal birth control you decide to use is personal to you.
It’ll depend on your preferences and goals – there is no right or wrong answer. If you’re unsure on which to use, speak to your GP.
If you’re unsure about using hormonal contraception all together, you can opt for non-hormonal alternatives, such as condoms and the copper coil.
How Do Hormonal Contraceptives Affect Women’s Hormones?
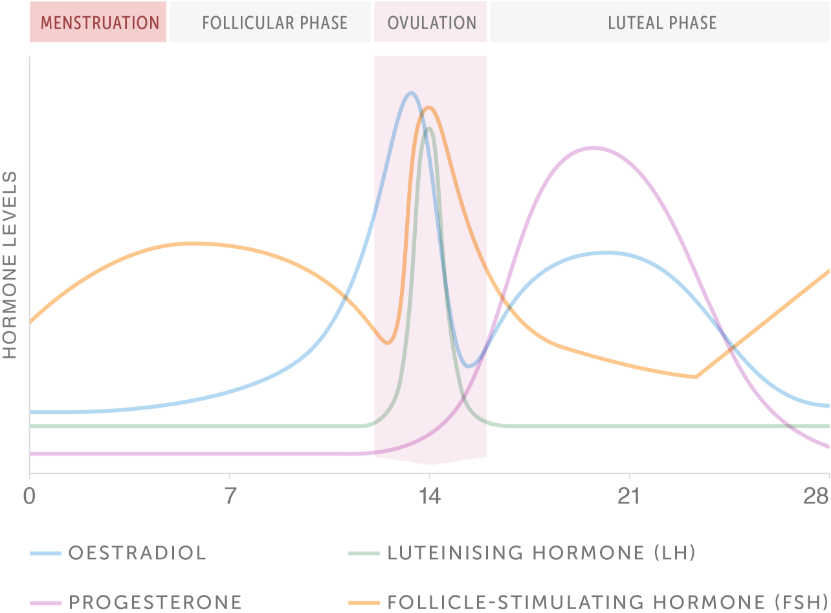
Your hormones naturally fluctuate across your menstrual cycle, rising and falling through each phase.
The four main hormones involved in the menstrual cycle are the two control hormones follicle-stimulating hormone and luteinising hormone, and the two ovarian response hormones oestrogen and progesterone.
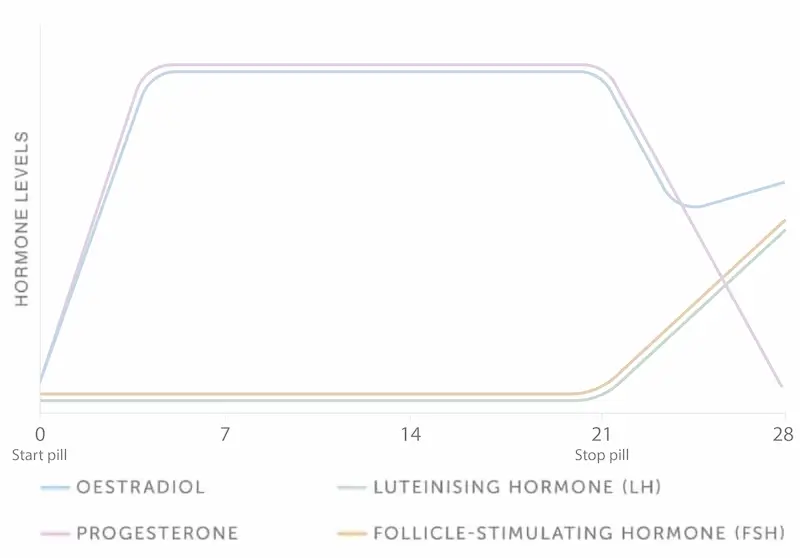
The natural fluctuation of your oestrogen and/or progesterone hormones is stopped when you use hormonal contraception.
The levels are kept constant instead, which suppresses the release of FSH and LH, stopping the natural menstrual cycle from happening[3] – see image below.
The combined oral contraceptive pill mimics a natural menstrual cycle as it’s taken daily for 3 weeks followed by a week of no pills. This causes what’s known as a withdrawal bleed or ‘break-through bleeding’ due to the drop in hormones.
Although it may seem a woman is having a ‘normal’ menstrual cycle, the high levels of Oestrogen and Progesterone prevent the natural menstrual cycle that underpins ovulation[3].
Essentially, hormonal contraceptives cause a hormone imbalance in women to prevent them from becoming pregnant.
The Side Effects of Hormonal Birth Control
Although they’re a great way of preventing pregnancy, hormonal contraceptives have a long list of side effects. Not everyone will experience the side effects to the same extent, and you may not have all of them, but it’s good to know what they are before you make the decision to use hormonal contraceptives. Some common side effects include:
Nausea: You may experience mild to moderate nausea, especially when you first start taking hormonal birth control. Taking it with food or at bedtime can help alleviate this side effect[4].
Breast Tenderness: Hormonal birth control can cause breast tenderness or enlargement in some people[5].
>Irregular Bleeding: Hormonal birth control can lead to irregular bleeding or spotting between periods, especially during the first few months of use. For some individuals, it can lead to lighter or even absent periods[6].
Headaches: Some people may experience headaches as a side effect of hormonal birth control[7].
Mood Changes: Hormonal changes can sometimes affect mood. You may experience mood swings, depression, or anxiety while using hormonal birth control[8].
Weight Changes: Although many studies have shown that hormonal contraception does not cause weight gain, the contraceptive injection has been shown to increase weight if taken for more than 2 years[9].
Decreased Libido: A decrease in sexual desire or changes in sexual function can happen when using hormonal birth control[10].
Vaginal Discharge: Some women may notice changes in vaginal discharge while using hormonal birth control[11].
Blood Pressure Changes: Hormonal birth control can, in rare cases, lead to an increase in blood pressure. Regular monitoring is essential for individuals at risk of hypertension[4].
Skin Changes: Changes in skin, such as acne improvement or worsening, is common while using hormonal birth control[12].
Blood Clots: There is a slight increased risk of blood clots with some hormonal birth control methods, particularly if you smoke or have a history of blood clots. This risk is higher with combined hormonal methods (containing both oestrogen and progestin) compared to progestin-only methods[4].
Cardiovascular Risk: Hormonal birth control may increase the risk of certain cardiovascular events, such as heart attack or stroke, particularly if you have preexisting risk factors. However, the risk is small for women under 35. Your doctor may be less likely to prescribe contraceptives with oestrogen if you have a history of heart disease[13].
Sleep problems: Hormonal contraception can cause people to have more REM sleep, meaning they’re more likely to suffer from poor sleep[14].
Does Birth Control Impact Mental Health?
There is some evidence suggesting that certain hormonal contraceptives, particularly those containing higher doses of oestrogen, may be associated with an increased risk of depression in some individuals[15]. However, the relationship between hormonal contraception and depression is complex and not fully understood.
Not all mental health effects of hormonal contraception are negative. Some women may experience improved mental well-being while using hormonal birth control. For example, some people find relief from mood-related symptoms, such as premenstrual dysphoric disorder (PMDD) or menstrual-related mood swings, when using hormonal contraception.
How to Start Hormonal Contraception
If you’re considering using hormonal contraception, there are a few steps you should take.
Firstly, research. Know how your hormones work across your menstrual cycle, how hormones support your health and wellbeing and the changes hormonal contraceptives have on your hormone network.
Once you understand this, you’re in a better position to make an informed decision on whether hormonal contraception is right for you. Then you can research the types of hormonal contraceptives, how they work and what their side effects are helping you make the right decision for you and your circumstances.
If you’re experiencing hormone related issues such as painful periods, heavy bleeding, or mood changes, it’s worth getting these investigated first. A good way to do this is with a hormone test for women. A hormone test can help identify the causes of these symptoms and rule out other conditions such as PCOS or endometriosis – going on hormonal contraception to relieve symptoms of these conditions prior to diagnosis will simply mask the condition.
Talking to a friend or relative about what contraception they use and how it affects them is a good way to get more information.
Your GP will also be able to help explain each type in more detail. They’ll also ask you questions to get a better understanding of which type would be best for you.
"There are lots of different options when it comes to HRT and it’s important you have a conversation with your GP about the symptoms that are bothering you most as sometimes the type of HRT you are given will vary based on this. Other things to consider are your lifestyle and how the type of HRT you’re taking can be incorporated into your life without being a burden."
If you’ve decided, for whatever reason, to come off hormonal contraception, what’s the best approach to take? And what are the likely side effects?
How Long Does It Take For Your Body To Get Back To Normal After Birth Control?
When you stop using hormonal birth control, it can take a few weeks for your body to get back to normal. Some women have a period between 2 and 4 weeks after stopping the pill but this can depend on the individual and their cycle. When you first stop taking the pill, it can take up to three months for your periods to become more regular. Therefore, it is important to give your body time to readjust and allow your cycle to re-establish itself.
When you stop taking the pill, the first period following is called a withdrawal bleed. The bleed after this one is your first natural period[4].
There is no evidence to suggest that the use of hormonal contraceptives negatively affects fertility[3]. In fact, some women fall pregnant immediately after they stop using birth control.
Side Effects of Stopping
Given the hormone changes that occur when you’re on hormonal contraception, it’s common to experience some side effects when you stop using hormonal contraceptives. This is due to your hormone fluctuations changing when you stop taking contraception resulting in your hormones reverting back to their natural fluctuating pattern across your menstrual cycle.
Some of the side effects you may experience as your hormones adjust back to their normal pattern include:
changes in the menstrual cycle
heavier periods
cramping during ovulation
premenstrual syndrome (PMS)
changes in mood
weight changes
acne
unwanted hair growth
headaches
tender breasts
changes in sex drive
The term “post-birth control syndrome” has been widely used on the internet and within the holistic world to describe the symptoms some women experience after coming off of hormonal contraception.
However, in the medical world, there is no evidence that such a condition exists. After stopping hormonal contraception, if your periods do not resume within 6 months you should consult your doctor for further investigations.
Equally, if you were prescribed hormonal contraception for reasons other than to prevent pregnancy, such as to treat acne, heavy periods, or conditions like PCOS, it is likely these pre-existing issues will return once you stop.
When To Seek Help
If you are struggling with the symptoms since stopping hormonal birth control, then you may need to seek medical advice.
Get To Know Your Hormones
If you are interested in finding out more about your natural hormone fluctuations across your entire menstrual cycle either before you start hormonal contraception or after stopping, then our advanced female hormone mapping test, MyFORM™, can help.
Unlike other female hormone tests, MyFORM® uses blood analysis and AI to map your hormones across your entire menstrual cycle. This will help you understand your hormones in much greater detail and allow you to build up a picture of your own, personal hormone fluctuations across your menstrual cycle. The detailed report will highlight any issues and can help identify hormone imbalance, meaning you can make more informed decisions about going on hormonal contraception.
MyFORM® is the only at-home blood test in the UK that maps all four key reproductive hormones across your entire menstrual cycle using two timed blood samples. Instead of a single snapshot, you get the full picture, personalised to your cycle, not a textbook average.
Multi-day test
MyFORM® Female Hormone Mapping
Understand your hormone patterns, ovarian response and menstrual cycle health with our ground-breaking hormone mapping test.
This information has been medically written by Dr Thom Phillips
Thom works in NHS general practice and has a decade of experience working in both male and female elite sport. He has a background in exercise physiology and has published research into fatigue biomarkers.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional
Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.